Retatrutide: The Next Generation of Weight Loss Injections
If you have been following developments in obesity medicine, you have likely heard whispers about retatrutide, sometimes branded as ‘Reta’. Pitched as the successor to Mounjaro and Wegovy, retatrutide is producing weight loss figures that, until recently, were the exclusive territory of bariatric surgery. Headlines have touted average reductions of nearly 30% of body weight in late-stage trials, prompting growing public interest and, unfortunately, a wave of unregulated online vendors.
But what exactly is retatrutide, where does it sit in the development pipeline, and when (if ever) will it become legally available in the UK? This guide unpacks the science, the trial data, the regulatory roadmap, and the critical question of how it compares to the injectables already on the market.

Quick summary
- Retatrutide is an investigational once-weekly injection developed by Eli Lilly.
- It activates three hormone receptors: GLP-1, GIP and glucagon, making it a ‘triple agonist’.
- Phase 3 trials show average weight loss of 28-30% over 68-104 weeks at the highest dose.
- It is not approved by the MHRA, FDA or EMA. Any product sold to UK consumers right now is unregulated and illegal.
- Realistic UK availability: late 2027 to mid-2028 privately, with NHS access unlikely before 2029.
What Is Retatrutide and How Does It Work?
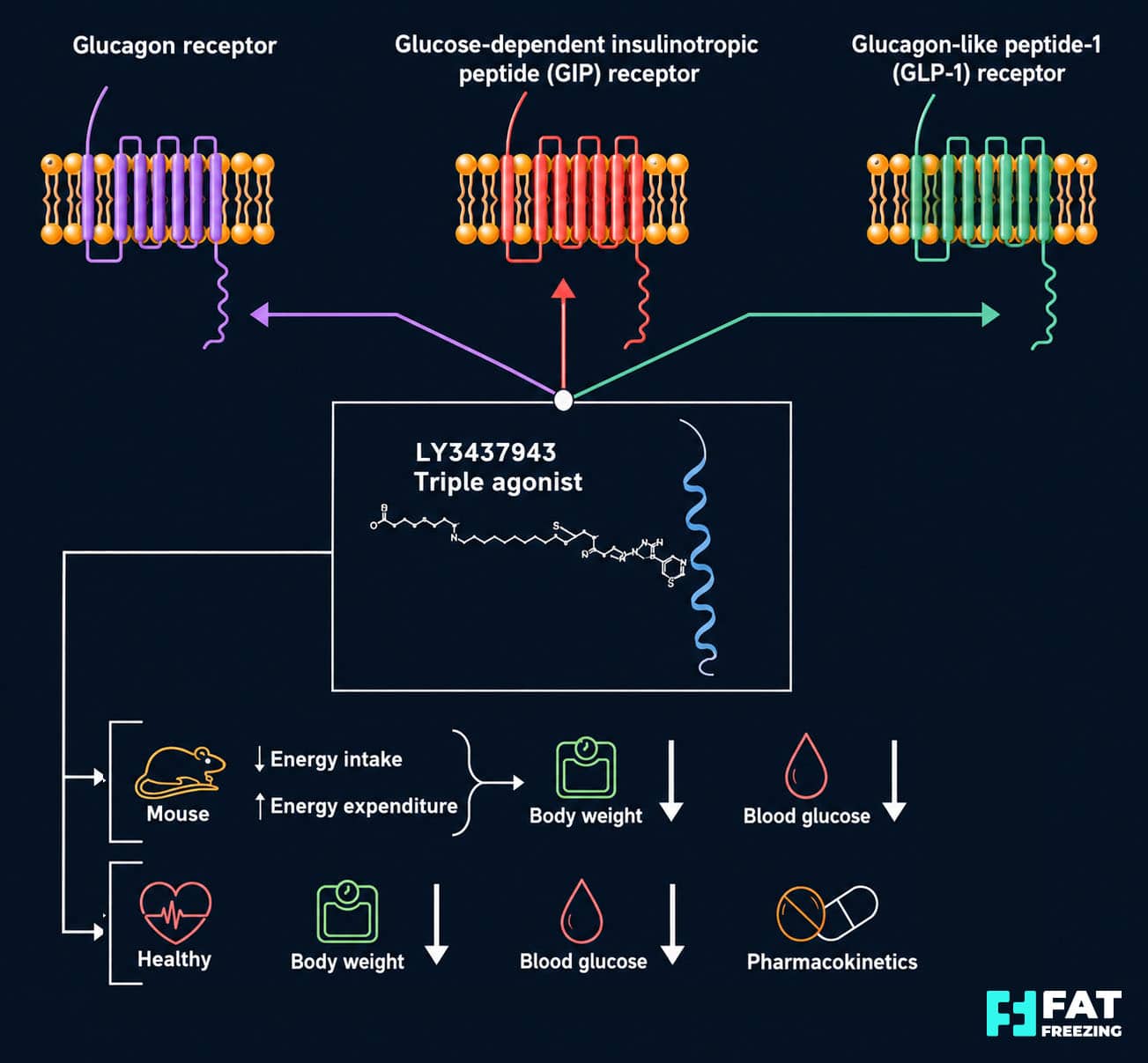
Retatrutide (development code LY3437943) is a 39-amino-acid peptide engineered to act simultaneously on three metabolic hormone receptors. To understand why this matters, it helps to track the evolution of incretin-based weight loss drugs.
Wegovy (semaglutide) targets a single receptor: GLP-1. It curbs appetite, slows gastric emptying and improves glycaemic control, producing roughly 14-19% weight loss over 68-72 weeks. Mounjaro (tirzepatide) goes a step further by hitting both GLP-1 and GIP receptors, achieving around 20-22.5% weight loss in comparable trials. Retatrutide adds a third axis: glucagon receptor activation.
The triple-agonist advantage
Each receptor contributes something distinct:
- GLP-1 activation reduces appetite, slows digestion and improves insulin response.
- GIP activation enhances satiety, supports insulin secretion and influences fat storage.
- Glucagon activation increases energy expenditure and stimulates fat oxidation in the liver and adipose tissue.
The clever bit is the balance. Retatrutide is tuned to be roughly 9 times more potent at the GIP receptor than native GIP, but slightly less potent than natural glucagon at its receptor, which prevents the unwanted hyperglycaemia you would otherwise expect from glucagon stimulation. The GLP-1 and GIP effects effectively chaperone the glucagon action, so you get the metabolic uplift without the blood sugar spike.
This is why retatrutide appears capable of doing something its predecessors cannot: it not only reduces calories in (appetite suppression) but also pushes calories out (increased energy expenditure). For a chronic, complex condition like obesity, that dual lever is significant.
What the Clinical Trials Show
Retatrutide’s trial data is, frankly, remarkable. Eli Lilly’s Phase 2 obesity study, published in the New England Journal of Medicine, set the tone: at 48 weeks, participants on the 12 mg dose lost an average of 24.2% of their starting body weight, compared with 2.1% on placebo. Notably, the weight-loss curve had not plateaued by week 48, hinting that the drug had more to give over longer periods.
Phase 3 results have since confirmed this trajectory.
TRIUMPH-4 (obesity with knee osteoarthritis)
Over 68 weeks, participants on 12 mg retatrutide lost an average of 28.7% of body weight, roughly 32 kg. Crucially, they also reported significant reductions in knee pain and improvements in physical function, suggesting benefits beyond the scale.
TRIUMPH-1 (broader obesity population)
At 80 weeks on 12 mg, mean weight loss was 28.3%, and 45.3% of participants achieved at least 30% weight loss, a threshold previously associated only with bariatric surgery. In a subgroup with severe obesity (BMI ≥35) who continued to 104 weeks, average weight loss reached 30.3%.
Type 2 diabetes (TRANSCEND-T2D-1)
In adults with type 2 diabetes, 12 mg retatrutide delivered approximately 16.8% weight loss and up to 2.0 percentage points reduction in HbA1c over 40 weeks, outperforming dulaglutide and placebo.
Fatty liver disease (MASLD)
Perhaps the most striking finding came from a dedicated Phase 2 substudy: at 24 weeks, retatrutide reduced liver fat by 82.4% at the 12 mg dose, with 86% of participants achieving normal liver fat content. For people living with metabolic dysfunction-associated steatotic liver disease, this is potentially transformative.
Retatrutide is the first pharmacologic treatment to routinely achieve bariatric-range weight loss in large, well-designed randomised trials, with nearly half of participants losing 30% or more of their starting weight.
Retatrutide vs Mounjaro vs Wegovy: How Do They Compare?
Direct head-to-head trials have not been published, so any comparison relies on cross-trial analysis. With that caveat, the picture looks something like this:
| Medication | Mechanism | Average Weight Loss | Trial Duration | UK Status |
|---|---|---|---|---|
| Wegovy (semaglutide) | GLP-1 agonist | ~14-19% | 68-72 weeks | MHRA approved |
| Mounjaro (tirzepatide) | GLP-1 / GIP dual agonist | ~20-22.5% | 72 weeks | MHRA approved, NHS rollout underway |
| Retatrutide (‘Reta’) | GLP-1 / GIP / glucagon triple agonist | ~24% at 48 weeks; ~28-30% at 68-104 weeks | 48-104 weeks | Investigational only, no approval |
On paper, retatrutide is the most potent of the three. But potency is not the only consideration. Retatrutide also produces a slightly more demanding side-effect profile, with notable rates of dysesthesia (skin tingling or burning) at higher doses, more pronounced heart rate increases, and similar or marginally higher rates of gastrointestinal symptoms compared to tirzepatide.
For an in-depth look at how the existing landscape compares to body-contouring alternatives, our guide on fat freezing versus Mounjaro walks through the trade-offs between pharmaceutical and non-invasive approaches.
Retatrutide: The Benefits and the Caveats
Potential Benefits
- Unprecedented average weight loss of 28-30% over 68-104 weeks at the highest dose
- Significant reductions in liver fat, with up to 86% achieving normal liver fat content
- Improvements in HbA1c, blood pressure, lipids and visceral adiposity
- Promising effects on knee osteoarthritis pain and obstructive sleep apnoea
- Once-weekly subcutaneous injection, similar in convenience to Wegovy or Mounjaro
- Triple-action mechanism addresses both calorie intake and energy expenditure
Important Considerations
- Not approved by the MHRA, FDA or EMA. Unavailable outside clinical trials
- Higher rates of nausea, vomiting and diarrhoea during dose escalation
- Dysesthesia (skin tingling) reported in roughly 1 in 5 patients at the 12 mg dose
- Modest heart rate increases of 5-10 bpm require monitoring
- Weight regain is likely if treatment is discontinued, suggesting long-term therapy
- Significant lean muscle loss alongside fat loss without proper diet and exercise support
- UK availability unlikely before late 2027 (private) or 2029 (NHS)
UK Regulatory Status: Where Are We Now?
This is where excitement needs to meet reality. As of 2026, retatrutide is not approved anywhere in the world. Eli Lilly has not yet submitted a New Drug Application to the FDA, let alone the MHRA. The current plan is to complete the Phase 3 TRIUMPH and TRANSCEND programmes through 2026, with regulatory submissions expected in late 2026 or early 2027.
Likely UK timeline
- Late 2026 / early 2027: Eli Lilly submits to the FDA and likely the MHRA shortly after.
- Late 2027 / mid-2028: Realistic window for MHRA marketing authorisation, assuming positive Phase 3 outcomes.
- 2028: Possible launch through regulated UK private clinics.
- 2029 onwards: Potential NHS availability, subject to NICE cost-effectiveness appraisal.
NICE will be the critical gatekeeper for NHS access. Given the cost of triple-agonist therapy and the size of the obese population, expect tight eligibility criteria, likely restricted initially to patients with severe obesity or significant comorbidities.
The grey market problem
You may have seen websites selling ‘retatrutide’ or ‘Reta’ peptides, often labelled ‘for research use only’. These products are unregulated, illegal to sell for human consumption, and potentially dangerous. The FDA has explicitly warned that retatrutide cannot be used in compounded products and has issued warning letters to vendors. The MHRA takes a similar view: any product sold in the UK as retatrutide outside of an approved clinical trial breaches medicinal product regulations.
The risks are not theoretical. These products may contain the wrong peptide sequence, incorrect dosing, bacterial contamination or unknown adulterants. Users are not screened for contraindications like a history of pancreatitis or medullary thyroid carcinoma, nor monitored for the cardiovascular, gallbladder or neurological side effects that can emerge during treatment.

What Should UK Patients Do Now?
If you are interested in retatrutide specifically, there are two legitimate paths.
1. Clinical trial participation
The TRIUMPH and TRANSCEND programmes include several UK sites. Trial participation offers free access to the investigational drug with comprehensive monitoring, though it requires randomisation (so you may receive placebo) and significant time commitment. ClinicalTrials.gov is the place to start.
2. Use what is already approved
For most people, the practical choice today is between MHRA-approved medications and other established interventions. Mounjaro and Wegovy already deliver substantial, evidence-based weight loss. Delaying treatment for years in the hope of accessing retatrutide carries its own health costs, particularly for those with existing comorbidities.
There are also non-pharmaceutical options worth considering, particularly for those who do not qualify for or do not wish to use injectable weight loss drugs. Fat freezing (cryolipolysis) remains the most widely used non-invasive body contouring treatment in the UK, targeting localised fat deposits without medication or downtime. For people who have already lost significant weight and want to address stubborn pockets, treatments like Aqualyx fat dissolving injections or EMSculpt for muscle toning may be appropriate adjuncts.
The reality is that obesity treatment is rarely about a single magic intervention. Our article on why losing weight is more difficult for some people explores the underlying biology, and the comparison piece Aqualyx vs Mounjaro may help you understand where different treatments fit within a broader plan.
The Bigger Picture
Retatrutide represents a genuine scientific leap. The fact that an injectable drug can produce surgical-range weight loss while improving liver fat, blood pressure, glycaemic control and joint pain marks a turning point in how obesity is treated.
But it also raises difficult questions. These drugs work for as long as you take them, so weight regain after discontinuation appears to be the rule rather than the exception. That means lifelong treatment for many, with the associated costs and ongoing risk of side effects. It also raises issues around equitable access, NHS budgeting, and the broader medicalisation of obesity in a society where food environment and lifestyle factors remain unaddressed.
For now, retatrutide is not a product you can buy. It is a powerful glimpse of where obesity medicine is heading, and a useful reminder that the safest, most effective path forward involves working with a regulated healthcare professional, evaluating all the available options, and making decisions grounded in evidence rather than hype.
Retatrutide is best understood today not as a product one can or should obtain in the UK, but as a powerful investigational tool reshaping expectations of what obesity treatment can achieve.
Frequently Asked Questions
Can I buy retatrutide legally in the UK right now?
No. Retatrutide is not approved by the MHRA, FDA or EMA, and cannot be legally prescribed in the UK on the NHS or privately. The only lawful way to receive retatrutide today is through enrolment in a regulated clinical trial. Any product marketed online as ‘retatrutide’ or ‘Reta’ for weight loss is unregulated and illegal to sell for human use, with significant safety risks including unknown purity, incorrect dosing and contamination.
When will retatrutide be available in the UK?
Realistic projections, assuming positive Phase 3 results and standard regulatory timelines, suggest MHRA marketing authorisation between late 2027 and mid-2028. Private UK availability could follow in 2028. NHS access via NICE appraisal is unlikely before 2029, and even then is likely to be restricted to patients with severe obesity or significant comorbidities. There is no credible pathway for legal UK availability in 2026 or early 2027.
How does retatrutide compare to Mounjaro for weight loss?
Cross-trial comparisons suggest retatrutide is more potent. Mounjaro (tirzepatide) 15 mg produces around 22.5% weight loss over 72 weeks, while retatrutide 12 mg achieves approximately 24% at 48 weeks and 28-30% by 68-104 weeks. However, retatrutide has not been compared head-to-head against Mounjaro, and it tends to cause more pronounced side effects such as dysesthesia (skin tingling) and larger heart rate increases. For now, Mounjaro remains the most effective licensed option available in the UK.
What are the main side effects of retatrutide?
The most common side effects are gastrointestinal: nausea, vomiting, diarrhoea and constipation, particularly during dose escalation. Dysesthesia, an abnormal tingling or burning sensation in the skin, affects roughly 1 in 5 patients on the 12 mg dose. Modest increases in resting heart rate (5-10 bpm) are typical. Like other GLP-1 class drugs, retatrutide carries theoretical risks of pancreatitis, gallbladder disease and, in susceptible individuals, medullary thyroid carcinoma. Long-term cardiovascular and renal safety is being evaluated in dedicated outcomes trials.
Will I need to take retatrutide forever?
Probably yes, if you want to maintain maximal weight loss. Long-term data on retatrutide is limited, but experience with semaglutide, liraglutide and tirzepatide consistently shows that weight regain begins within weeks of stopping treatment, regardless of how long someone has been on the drug. The underlying biology of appetite and energy regulation reasserts itself once pharmacological support is removed. Most experts now view incretin-based therapy as long-term chronic disease management, similar to ongoing antihypertensive treatment.
Are there alternatives to weight loss injections?
Yes. For people who do not qualify for, cannot tolerate or do not wish to use injectable weight loss medications, there are several evidence-based alternatives. Non-invasive body contouring treatments like fat freezing (cryolipolysis) target localised fat deposits without medication, while options like fat-dissolving injections, ultrasound cavitation and muscle-toning technologies such as EMSculpt can address specific aesthetic concerns. Bariatric surgery remains the most powerful intervention for severe obesity. Structured lifestyle programmes, often combined with one of the above, continue to form the foundation of sustainable weight management.
